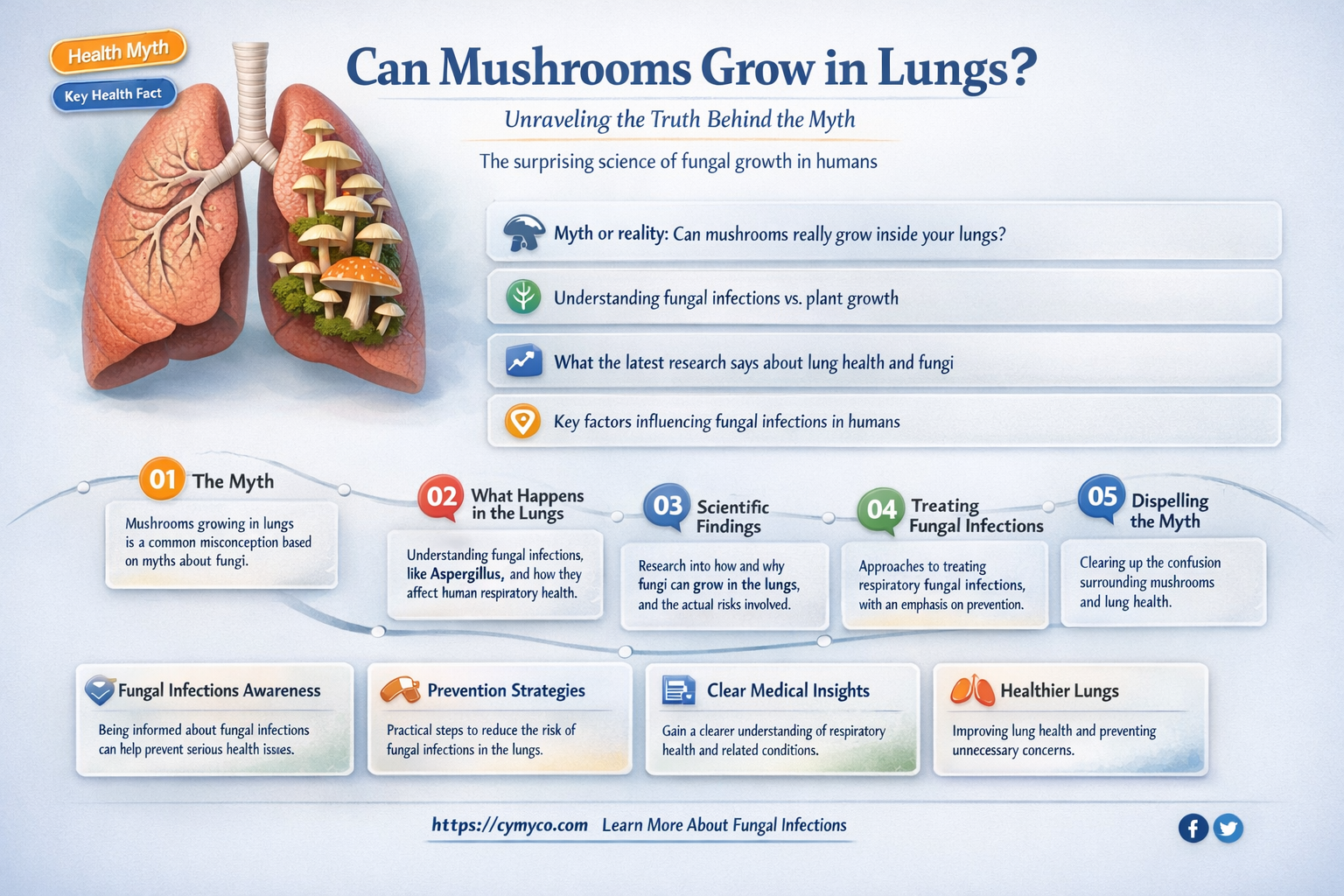
The idea of mushrooms growing in human lungs may seem like something out of a science fiction novel, but it is a topic that has sparked curiosity and concern among medical professionals and the general public alike. While it is not common, there have been rare and alarming cases where fungal infections, particularly those caused by Aspergillus, have led to the growth of mold-like structures in the lungs, resembling mushrooms. These infections, known as aspergillomas, typically occur in individuals with pre-existing lung conditions or weakened immune systems, raising questions about the potential risks and implications of such unusual fungal growths within the human body.
| Characteristics | Values |
|---|---|
| Can mushrooms grow in lungs? | No, mushrooms cannot grow in human lungs under normal circumstances. |
| Reason for impossibility | Human lungs lack the necessary environment (soil, moisture, nutrients) for fungal growth. |
| Related medical condition | Aspergilloma (fungal ball) can form in lungs, but it is not a mushroom; it is caused by Aspergillus fungus. |
| Misconception origin | Likely from fictional or exaggerated stories, as fungi require specific conditions not present in lungs. |
| Potential for fungal infections | Yes, but these are typically caused by molds or yeasts, not mushrooms. |
| Examples of lung fungi | Aspergillus, Candida, Cryptococcus (not mushrooms). |
| Treatment for lung fungal infections | Antifungal medications, surgery in severe cases (e.g., aspergilloma). |
| Prevention | Avoid environments with high fungal spore counts, treat underlying conditions like immunodeficiency. |
| Scientific consensus | Mushrooms growing in lungs is biologically implausible and not documented in medical literature. |
Explore related products






What You'll Learn
- Spores Inhalation Risks: Can airborne mushroom spores enter lungs and cause infections or growth
- Mycetoma in Lungs: Fungal masses forming in lung tissue due to spore colonization
- Immune System Role: How immunity prevents or allows mushroom growth in lung environments
- Medical Case Studies: Documented instances of fungal growth in human lungs
- Prevention Strategies: Methods to avoid inhaling spores and lung fungal infections
![]()
Spores Inhalation Risks: Can airborne mushroom spores enter lungs and cause infections or growth?
Airborne mushroom spores are ubiquitous in the environment, especially in areas with high humidity and organic matter. While these spores are generally harmless to healthy individuals, their inhalation raises questions about potential risks, particularly whether they can enter the lungs and cause infections or growth. The respiratory system is designed to filter out foreign particles, but certain conditions may allow spores to bypass these defenses. For instance, individuals with compromised immune systems, chronic lung diseases, or those exposed to high concentrations of spores are at greater risk. Understanding the mechanisms of spore inhalation and the body’s response is crucial for assessing these risks.
Inhalation of mushroom spores can lead to pulmonary complications in specific circumstances. One well-documented condition is allergic bronchopulmonary mycosis (ABPM), which occurs when repeated exposure to fungal spores triggers an allergic reaction in the lungs. Symptoms include wheezing, coughing, and shortness of breath. While this is not an infection, it highlights the body’s sensitivity to fungal particles. More severe cases involve fungal pneumonia, where spores colonize lung tissue, typically in immunocompromised individuals. For example, species like *Aspergillus* and *Candida* are known culprits, but common mushroom spores are rarely implicated. Dosage matters here: prolonged exposure to high spore counts in enclosed spaces, such as mushroom farms, increases the likelihood of adverse effects.
The idea of mushrooms growing in the lungs is largely a myth, but it stems from rare, sensationalized cases. One such instance involved a man with chronic obstructive pulmonary disease (COPD) who developed a fungal ball in his lung after inhaling *Candida* spores. However, this is not typical of mushroom spores, which lack the biological mechanisms to establish growth in human tissue. Mushroom mycelium requires specific substrates, such as wood or soil, to thrive, which the lung environment does not provide. Thus, while spores may colonize under extreme conditions, actual mushroom growth in the lungs is biologically implausible.
Practical precautions can minimize spore inhalation risks. For individuals working in mushroom cultivation or living in mold-prone environments, wearing N95 masks reduces spore exposure. Maintaining indoor humidity below 50% discourages fungal growth, and regular ventilation prevents spore accumulation. Immunocompromised individuals should avoid areas with visible mold or mushroom growth. If respiratory symptoms develop after spore exposure, seeking medical attention is critical, as early intervention can prevent complications. While the risk of lung infections from mushroom spores is low, awareness and preventive measures are key to respiratory health.
Can Mushrooms Grow in Human Flesh? Unraveling the Myth and Science
You may want to see also
Explore related products






![]()
Mycetoma in Lungs: Fungal masses forming in lung tissue due to spore colonization
Fungal infections in the lungs are a rare but serious concern, and mycetoma represents one of the most unusual manifestations. Unlike typical pneumonia or aspergillosis, mycetoma involves the formation of granular masses within lung tissue, often caused by the colonization of spores from fungi like *Madurella* or *Pseudallescheria*. These masses, known as grains, can mimic tumors on imaging, leading to diagnostic challenges. While mycetoma is more commonly associated with subcutaneous infections, pulmonary involvement occurs when spores are inhaled and establish a foothold in the lung parenchyma, particularly in individuals with compromised immunity or pre-existing lung conditions.
The development of mycetoma in the lungs follows a distinct pathophysiology. Spores inhaled from the environment evade the immune system and germinate within the alveoli, forming hyphae that aggregate into grains. Over time, these grains enlarge, triggering a chronic inflammatory response. The body’s attempt to wall off the infection results in fibrosis and cavitation, which can lead to symptoms like chronic cough, hemoptysis, and chest pain. Unlike superficial mycetoma, pulmonary cases are often asymptomatic in early stages, making detection difficult until complications arise, such as bronchial obstruction or secondary bacterial infections.
Diagnosing pulmonary mycetoma requires a combination of clinical suspicion, imaging, and microbiological confirmation. High-resolution CT scans typically reveal nodular or cavitary lesions with calcifications, but these findings are not pathognomonic. Definitive diagnosis hinges on histopathological examination of biopsy samples, where grains stained with periodic acid-Schiff (PAS) or Gomori methenamine silver (GMS) highlight fungal elements. Culture of the causative organism is essential for species identification, though it may take weeks due to the slow-growing nature of many fungi involved. Molecular techniques like PCR are increasingly valuable for rapid and accurate identification.
Treatment of pulmonary mycetoma is complex and often protracted. Surgical excision, the mainstay for subcutaneous mycetoma, is rarely feasible in the lungs due to the risk of hemorrhage and pneumothorax. Instead, antifungal therapy forms the cornerstone of management, with agents like itraconazole, posaconazole, or amphotericin B tailored to the identified species. Treatment duration typically spans 6 to 12 months, with response monitored via imaging and clinical improvement. Adjunctive measures, such as bronchoscopic debridement or immunomodulators, may be considered in refractory cases. Early intervention is critical, as untreated pulmonary mycetoma can progress to respiratory failure or disseminate to other organs.
Preventing pulmonary mycetoma hinges on minimizing exposure to fungal spores, particularly in endemic regions like Africa, India, and Latin America. Individuals with occupational or environmental risk factors, such as farmers or construction workers, should use protective masks in dusty settings. For immunocompromised patients, prophylactic antifungal therapy may be warranted. Public health efforts should focus on raising awareness among healthcare providers, as misdiagnosis is common. While pulmonary mycetoma remains a rare entity, its potential for morbidity underscores the importance of vigilance and prompt, targeted management.
Mushrooms in Coal Dust: Unlikely Growth or Ecological Innovation?
You may want to see also
Explore related products






![]()
Immune System Role: How immunity prevents or allows mushroom growth in lung environments
The human immune system is a formidable defense mechanism, constantly patrolling the body for foreign invaders. In the context of mushroom growth in the lungs, this system plays a pivotal role in determining whether such an unusual scenario could ever become a reality. Immune cells, particularly macrophages and neutrophils, act as the first line of defense, swiftly identifying and engulfing any foreign particles, including fungal spores, that enter the respiratory tract. This rapid response is crucial, as it prevents the spores from germinating and establishing a foothold in the lung tissue. For instance, when a person inhales mold spores, which are structurally similar to mushroom spores, the immune system's immediate reaction often leads to their elimination before they can cause any harm.
A healthy immune system is adept at recognizing and responding to fungal threats. It employs a multi-pronged approach, including the production of antimicrobial proteins and the activation of specific immune cells like T-helper 17 (Th17) cells, which are essential for combating fungal infections. These Th17 cells secrete cytokines, signaling molecules that recruit other immune cells to the site of infection, creating an inhospitable environment for fungal growth. This intricate immune response is why, despite the presence of fungal spores in the air we breathe, healthy individuals rarely experience fungal infections in their lungs, let alone the growth of mushrooms.
However, the immune system's effectiveness can be compromised, creating opportunities for fungal infections to take hold. Immunocompromised individuals, such as those undergoing chemotherapy, living with HIV/AIDS, or taking immunosuppressive medications after organ transplants, face a higher risk. In these cases, the immune system's ability to detect and destroy fungal invaders is diminished, allowing spores to germinate and potentially develop into more complex structures. For example, *Pneumocystis jirovecii*, a fungus that can cause severe pneumonia in immunocompromised patients, highlights how a weakened immune response can lead to fungal proliferation in the lungs.
The environment within the lungs also plays a critical role in this dynamic. The warm, moist conditions of the respiratory tract are not inherently conducive to mushroom growth, as mushrooms typically require specific substrates and environmental conditions to thrive. However, in cases of severe immune suppression, the lungs can become a more permissive environment. Practical measures to support immune health, such as maintaining a balanced diet rich in vitamins and minerals, regular exercise, and adequate sleep, can bolster the body's defenses. For immunocompromised individuals, healthcare providers may recommend prophylactic antifungal medications, such as trimethoprim-sulfamethoxazole, to prevent fungal infections, including those that could theoretically lead to mushroom-like growths.
In summary, the immune system's vigilance and adaptability are key to preventing mushroom growth in the lungs. While the idea of mushrooms growing in this environment remains largely within the realm of science fiction, understanding the immune system's role provides valuable insights into how the body protects itself from fungal threats. By supporting immune health and taking proactive measures, especially in vulnerable populations, we can further reduce the already minuscule risk of such extraordinary biological phenomena.
Can Mushrooms Grow in Intestines? Debunking Myths and Facts
You may want to see also
Explore related products





![]()
Medical Case Studies: Documented instances of fungal growth in human lungs
Fungal growth in human lungs, though rare, is a documented phenomenon with severe implications for patient health. Medical case studies reveal instances where fungi, particularly species like *Aspergillus* and *Candida*, have colonized lung tissue, often in immunocompromised individuals. These cases highlight the importance of early detection and targeted treatment to prevent life-threatening complications such as invasive aspergillosis or candidiasis. Understanding these documented instances provides critical insights into risk factors, diagnostic methods, and therapeutic strategies.
One notable case study involves a 45-year-old male with chronic obstructive pulmonary disease (COPD) who developed *Aspergillus fumigatus* colonization in his lungs. The patient presented with persistent cough, hemoptysis, and weight loss. A high-resolution CT scan revealed a fungal ball (aspergilloma) in a pre-existing lung cavity, a common site for fungal growth due to poor ventilation and mucus accumulation. Treatment included antifungal therapy with voriconazole (200 mg twice daily) and surgical resection of the cavity to prevent further dissemination. This case underscores the role of pre-existing lung conditions in predisposing individuals to fungal infections.
In contrast, a 28-year-old female with acute myeloid leukemia (AML) developed invasive pulmonary aspergillosis during chemotherapy-induced neutropenia. Her symptoms included fever, dyspnea, and chest pain. Diagnosis was confirmed via galactomannan antigen testing and bronchoalveolar lavage. Liposomal amphotericin B (3 mg/kg/day) was initiated, followed by posaconazole (300 mg twice daily) for consolidation therapy. This case illustrates the heightened risk in immunocompromised patients and the necessity of prompt, aggressive antifungal treatment.
A comparative analysis of these cases reveals distinct patterns. The COPD patient’s infection was localized and manageable with surgery, whereas the AML patient’s systemic involvement required prolonged antifungal therapy. Both cases emphasize the importance of tailoring treatment to the patient’s immune status and the extent of fungal invasion. Additionally, prophylactic antifungal measures, such as posaconazole for high-risk hematology patients, can reduce the incidence of invasive fungal infections.
Practical tips for healthcare providers include monitoring high-risk patients (e.g., those with COPD, HIV, or undergoing chemotherapy) for early signs of fungal infection, such as persistent respiratory symptoms or fever. Diagnostic tools like CT scans, serum biomarkers, and microbiological cultures should be employed promptly. Patients should be educated on environmental risk factors, such as exposure to moldy environments, and advised to avoid such settings. By integrating these strategies, clinicians can mitigate the risks and improve outcomes for patients at risk of pulmonary fungal growth.
Can Mushrooms Thrive in Dog Poop? Surprising Facts Revealed
You may want to see also
Explore related products






![]()
Prevention Strategies: Methods to avoid inhaling spores and lung fungal infections
While mushrooms growing in lungs is an extremely rare occurrence, inhaling fungal spores can lead to serious lung infections, particularly in immunocompromised individuals. Understanding how to minimize spore exposure is crucial for preventing these infections.
One key strategy is environmental control. Mold thrives in damp, humid environments. Maintaining indoor humidity below 50% using dehumidifiers, promptly fixing leaks, and ensuring proper ventilation in bathrooms and kitchens significantly reduces spore presence. Regularly cleaning areas prone to moisture, like shower curtains and window sills, is essential.
Personal protective measures are another vital layer of defense. When engaging in activities that disturb soil or decaying organic matter, such as gardening, construction, or hiking in wooded areas, wearing a mask rated N95 or higher effectively filters out fungal spores. This is especially important for individuals with weakened immune systems or pre-existing lung conditions.
Lifestyle choices also play a role. Avoiding smoking is paramount, as it damages the lungs' natural defenses, making them more susceptible to infection. A balanced diet rich in fruits, vegetables, and whole grains supports a healthy immune system, enhancing the body's ability to combat fungal invaders.
Finally, medical vigilance is crucial. Individuals undergoing immunosuppressive therapies, such as chemotherapy or organ transplant recipients, should be under close medical supervision. Prophylactic antifungal medications may be prescribed in high-risk situations. Early detection and treatment of fungal infections are essential for successful outcomes.
Mushrooms in Horse Manure: Unveiling the Surprising Growth Potential
You may want to see also
Frequently asked questions
While extremely rare, there have been documented cases of fungal infections in the lungs, such as aspergillosis, where fungi can colonize lung tissue. However, true mushrooms (basidiomycetes) do not grow in human lungs; these cases typically involve molds or other fungi.
Fungal infections in the lungs, like aspergillosis or histoplasmosis, are caused by inhaling fungal spores from the environment. They can be dangerous, especially for individuals with weakened immune systems, and may require antifungal treatment.
No, eating contaminated or poisonous mushrooms does not cause mushrooms to grow in the lungs. Ingesting toxic mushrooms can lead to poisoning or organ damage, but it does not result in fungal growth in lung tissue.



























